Introduction:
Light chain amyloidosis (AL) is a plasma cell disorder associated with detrimental manifestations in multiple organ systems of the body. It is estimated that approximately 1275-3200 new cases occur in the United States annually. Proteasome inhibitors (PI), such as bortezomib, carfilzomib, and ixazomib used for multiple myeloma treatment are also used for the treatment of AL amyloidosis. Our aim in this review is to evaluate the efficacy and safety profile of PI-based regimens for the treatment of newly diagnosed AL Amyloidosis (ND-AL).
Methods:
We conducted a systematic review (following PRISMA guidelines) by completing a comprehensive literature search on PubMed, Cochrane, ClinicalTrials.gov, and Embase on June 23rd, 2020. We were able to identify 901 articles, 325 articles from PubMed, 50 from Cochrane, 23 from Clinical Trials.org, and 253 from Embase. After the screening, we selected 11 published studies (n=436) including 5 phase lll trials, 2 phase I/II trials.
Results:
Cyclophosphamide, Bortezomib, Dexamethasone (CyBorD) with or without Daratumumab (Dara):
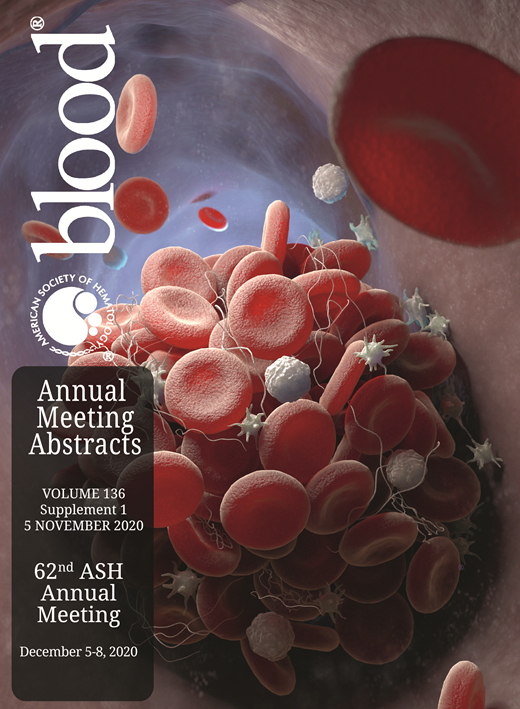
In a Phase lll trial (ANDEROMADA study), Palldini et al. (2020) studied the efficacy of Dara+ CyBorD vs CyBorD in ND-AL pts (n=28). The addition of Dara to CyBorD showed an improved overall hematological response (ORR) in 96% with complete response (CR) in 54% pts at a median follow up of 17.6 months (Table 1).
In a retrospective study by Lim et al. (2017), CyBorD was given to ND-AL pts (n=39) which showed an ORR in 63% with very good partial response (VGPR) in 50% pts.
In a retrospective study by Diaz-Pallares et al. (2020), CyBord was given to ND-AL pts (n=34) which showed an ORR in 91% with CR, VGPR, and partial response (PR) in 26%, 26%, and 38% pts, respectively. Progression-free survival (PFS) and overall survival (OS) were reported at 26.7 months and 22 months (P=0.06) respectively (Table 1).
Bortezomib, Melphalan, Dexamethasone (BMD):
In a phase III trial (EMN-03 study), Kastritis et al. (2020) studied the efficacy of BMD vs MD in ND-AL pts (n=109). Addition of B to MD showed an improved ORR: 81% vs 56% (p=0.001) with CR/VGPR in 53% vs 28% pts. No significant difference in survival outcome was observed.
In a phase III trial, Kastritis et al. (2015) studied the efficacy of BMD vs MD in ND-AL pts (n=69). Addition of B to MD showed an improved ORR: 75% vs 53% (p=0.075) with CR/VGPR in 56% vs 42% pts (p=0.277). OS and PFS were also improved in BMD group as compared to control group: 83% vs 72% (p= 0.295) and 61% vs 49% (p=0.079) at 2 years, respectively (Table 1).
Bortezomib, Melphalan, Prednisolone (BMP):
In a retrospective study by Lee et al. (2014), BMP was given to ND-AL pts (n=19) which showed an ORR in 84% pts with CR, VGPR and PR in 37%, 21% and 26% pts, respectively (Table 1).
Induction with B based regimens for ASCT:
In a Phase lll trial (HOVON 104), Minnema et al. (2019), studied the efficacy of BD induction prior to HDM/ASCT in pts (n=35) with ND-AL. At 6 months, BD induction prior to HDM/ASCT vs No BD Induction prior to HDM/ASCT showed an ORR: 80% vs 80% with an improved CR: 43% vs 5% and VGPR: 54% vs 51%.
In a Phase I/II trial by Sanchorawala et al. (2015), BD induction followed by B-HDM conditioning for ASCT was done in pts (n=27) with ND-AL. ORR at 6 months post ASCT was observed in 100% pts with CR and VGPR in 63% and 37% pts, respectively (Table 1).
Induction with B based regimen prior to ASCT vs Upfront ASCT:
In a retrospective analysis by Scharman et al. (2017), 53 pts who received ASCT were categorized into 3 groups i.e. Upfront ASCT, induction with B based regimen and induction with other regimens. ND-AL Patients (n=34/53) receiving B based induction vs no induction showed an improved ORR: 94% vs 69% (p=0.04). OS also improved in B based induction as compared to no induction group: 87% vs 77% (p=0.22) at 3 years. PFS at 3 years was 61% vs 69%, respectively (Table 1).
Conclusions:
PI-based regimens have shown favorable outcomes in the treatment of ND-AL and are effective therapeutic options. The most promising results are observed with CyBorD+Dara. The adverse events associated with PI-based therapy are peripheral neuropathy, anemia, thrombocytopenia, and infections. Further prospective clinical trials are warranted for a broader understanding of the safety and efficacy profile of PI-based regimens and correlation with individual pts characteristics.
Table Caption:
Table 1: Comparative efficacy and safety of proteasome-inhibitor based drug regimens in ND-AL
Anwer:Incyte, Seattle Genetics, Acetylon Pharmaceuticals, AbbVie Pharma, Astellas Pharma, Celegene, Millennium Pharmaceuticals.: Honoraria, Research Funding, Speakers Bureau.